- Ankle Arthritis
- Anterior Ankle Impingement and Bone Spurs
- Posterior Ankle Impingement and Os Trigonum
- Ankle Fracture
- Ankle Instability
- Ankle Syndesmosis Injury
- Osteochondral Lesions of the Talus (OLT)
- Tibialis Posterior Tendon Dysfunction
- Plantar Fasciitis
- Hindfoot Arthritis
- Lesser Toe Deformity
- Achilles Tendon Disorders
- Achilles Tendon Rupture
- Peroneal Tendon Disorders
- Calf Strain
- Ganglions
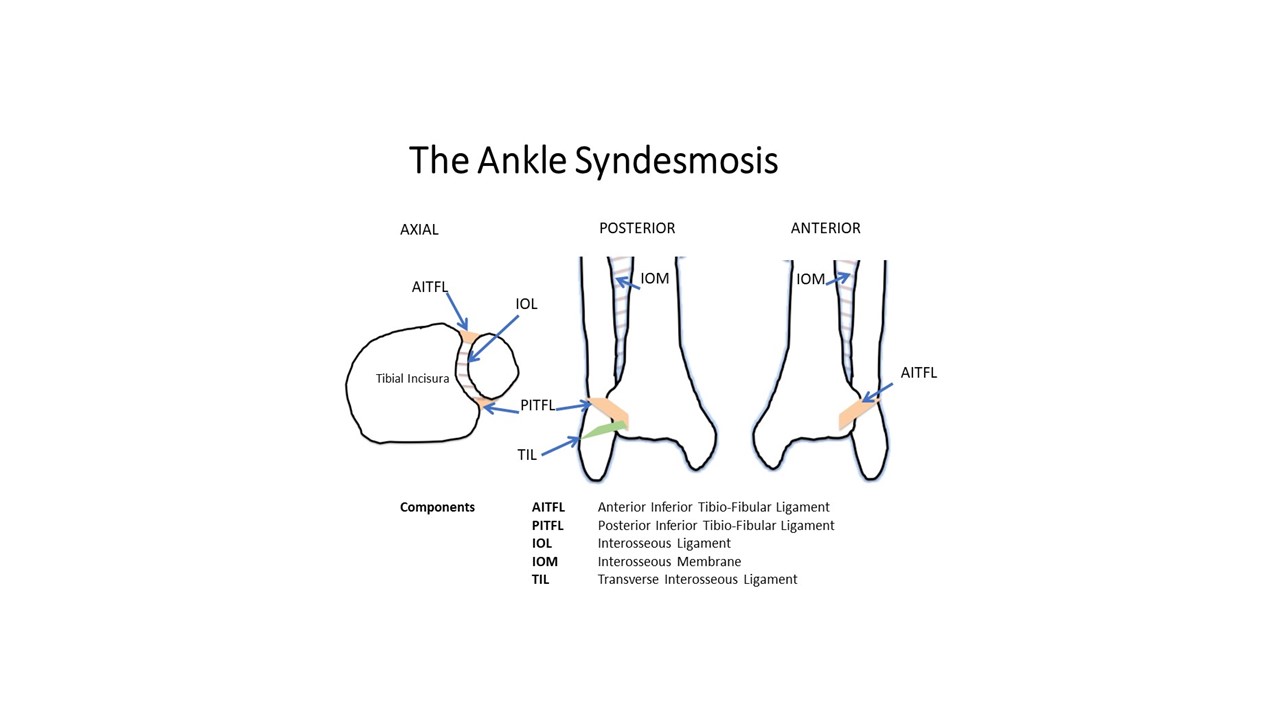
Ankle Syndesmosis Injury / High Ankle Sprain
What is it?
The ankle syndesmosis is a collection of strong ligaments that bind the tibia and fibula together thereby establishing their close relationship at the ankle joint. The syndesmosis has a crucial role in maintaining ankle stability and normal function. An injury of the ankle syndesmosis is not always accompanied by an ankle fracture and is not always obvious on X-ray, therefore a high degree of clinical suspicion with thorough examination and imaging is needed to exclude it.
What is it caused by?
Predictable patterns of ankle injury cause a syndesmosis injury. Most commonly a twisting and abduction mechanism (ankle and foot turn and rotate outwards) such as those that can occur in football/rugby players when tackled while their foot is fixed on soft ground by virtue of their boot studs. This can also be the case when tackles are made on Astroturf.
Symptoms
Pain, swelling and bruising, higher around the ankle compared with a standard ankle sprain is usual. The pain may infact be apparent us far up as the knee since the syndesmosis is a continuous structure all the way throughout the lower leg.
Syndesmosis injuries are frequently missed and commonly present to the foot and ankle clinic some time after the initial injury. Patients with chronic syndesmosis report ankle pain with activity, difficulty returning to sport, difficulty balancing on the ankle and lateral-sided ankle pain.
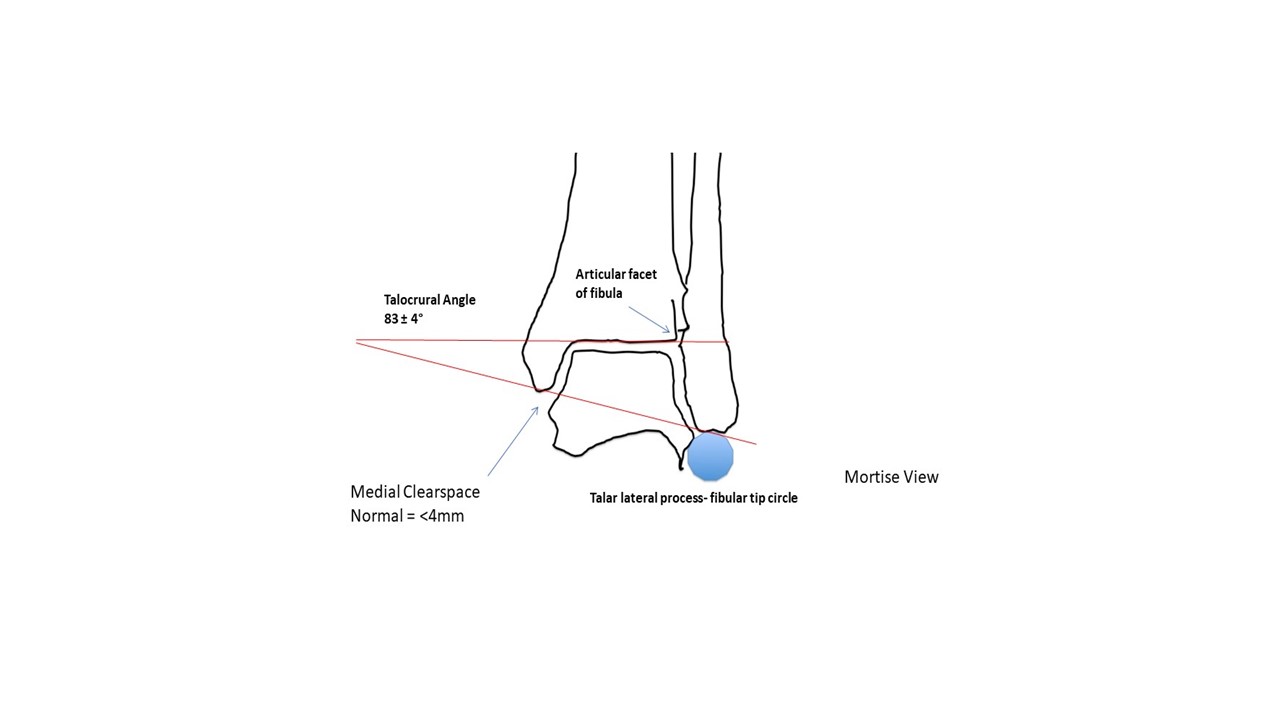
Diagnosis
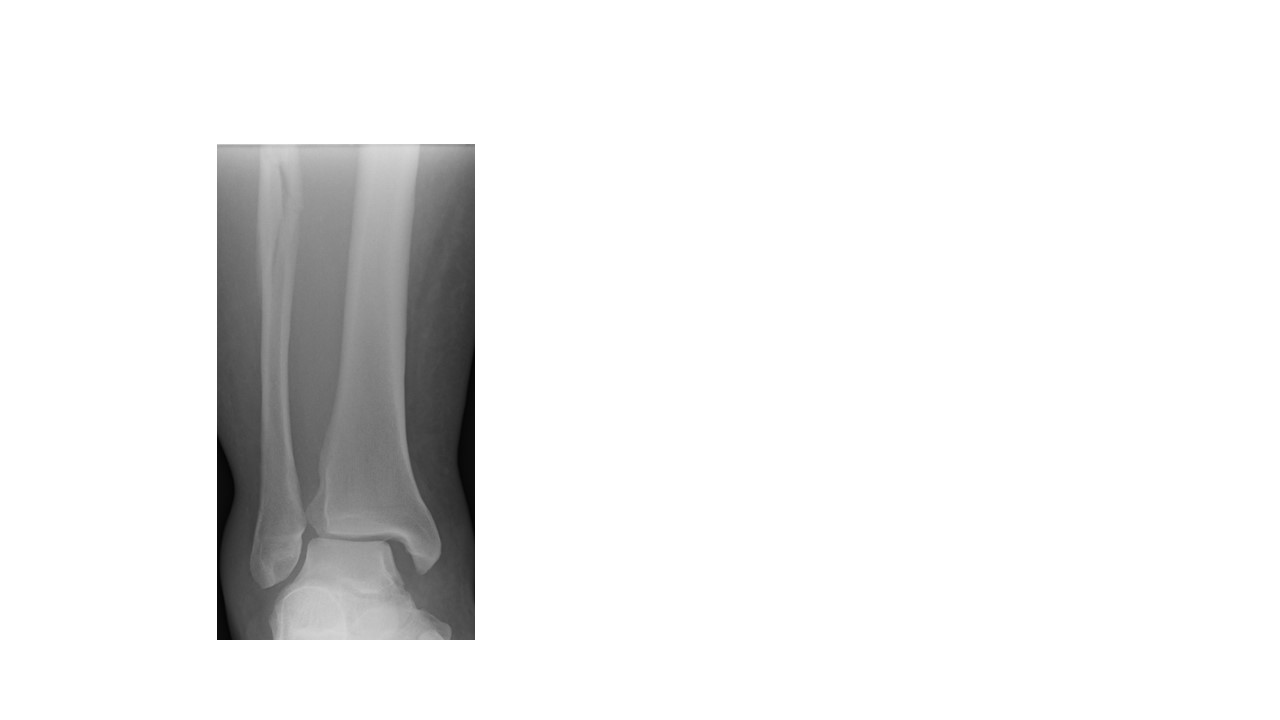
We employ our experience as well as established normal reference values on plain X-ray. These will help determine whether there is an obvious syndesmosis injury or highlight a particular fracture pattern that is highly predictive of a syndesmosis injury such as the high fibular fracture ( a “Maisonneuve injury”) above the ankle syndesmosis (shown below).
More subtle syndesmosis injuries require cross-sectional imaging- either or both MRI and standing CT scanning.
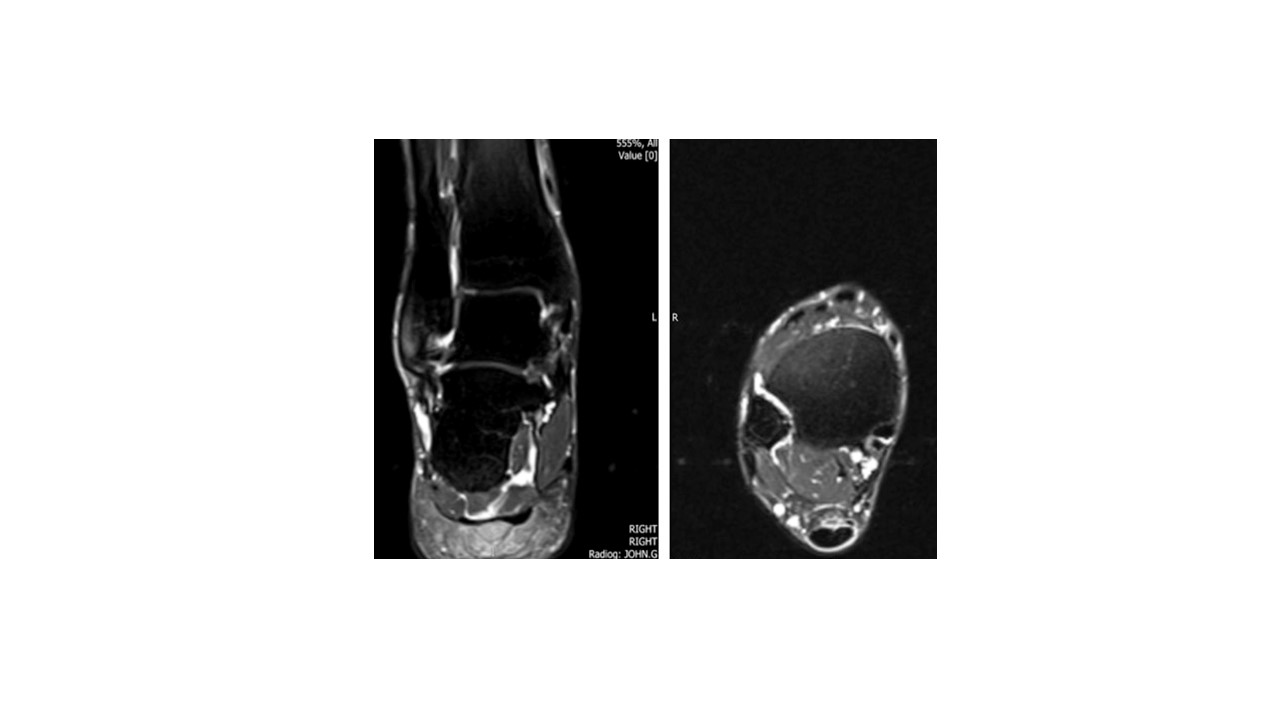 MRI- fluid-weighted sequence showing coronal (frontal) and axial (transverse) slices through the ankle joint at the level of ankle syndesmosis where the front, intermediate and posterior syndesmotic ligaments are torn- demonstrated by the tracking ankle effusion.
MRI- fluid-weighted sequence showing coronal (frontal) and axial (transverse) slices through the ankle joint at the level of ankle syndesmosis where the front, intermediate and posterior syndesmotic ligaments are torn- demonstrated by the tracking ankle effusion.
Non-Surgical Treatment
As with many injuries, provided timely management is implemented, relative success with non-operative treatment can be anticipated. Unfortunately with late-presenting injuries the success of non-operative treatment can be limited. Bracing and physio-taping circumferentially around the ankle can offer symptomatic benefit and is also useful as a clinical test of stability. Ultimately these are injuries that very often require surgery.
Surgical
The method of surgical treatment depends on injury chronicity. Unstable, yet well-aligned syndemoses presenting within 3 months of injury require little more than arthroscopic “freshening” of the of the internal syndesmotic ligaments to create adhesion and stabilization with flexible suture-buttons or tightropes (shown below).

I have a particular interest in revision work and salvaging chronic injury and have employed other techniques, all with the aim of establishing perfect ankle anatomy and minimizing the risk of future arthritis.





