- Ankle Arthritis
- Anterior Ankle Impingement and Bone Spurs
- Posterior Ankle Impingement and Os Trigonum
- Ankle Fracture
- Ankle Instability
- Ankle Syndesmosis Injury
- Osteochondral Lesions of the Talus (OLT)
- Tibialis Posterior Tendon Dysfunction
- Plantar Fasciitis
- Hindfoot Arthritis
- Lesser Toe Deformity
- Achilles Tendon Disorders
- Achilles Tendon Rupture
- Peroneal Tendon Disorders
- Calf Strain
- Ganglions
Anterior Ankle Impingement & Bone Spurs
Ankle impingement describes the symptom of pain emerging from the margins of the joint due to pinching of tissue. It is most common at the front of the ankle when it is termed “anterior ankle impingement” but it can also at the back or sides of the ankle.
What is it caused by?
Marginal spurs of bone and cartilage can form due to repeated injuries to the ankle when the cartilage is damaged. These spurs can irritate and even trap the overlying soft tissues in the joint, causing pain on extremes of ankle motion.
Symptoms
A history of repeated ankle sprains is very common. The condition is sometimes called a “footballer’s ankle” for this reason. Ankle instability or structural deformity around the ankle can cause impingement as well as primary disorders and inflammation of the lining of the ankle joint capsule, the “synovium”.
Patients may have swelling in the ankle and a catching sensation with certain movements such as when climbing stairs, kneeling or jumping. A limp may be apparent with severe inflammation in the ankle.
Diagnosis
Impingement can occur in patients known to have ankle arthritis, but it is important to differentiate between patients with and without arthritis as the treatment and prognosis is different.
Clinical examination of the ankle to identify positional restrictions as well as a special test to simulate the impingement is diagnostic as impingement is a functional problem, apparent with movement. Standing X-rays of the ankle will show large bone spurs but cross-sectional imaging with MRI or CT scanning is often needed.
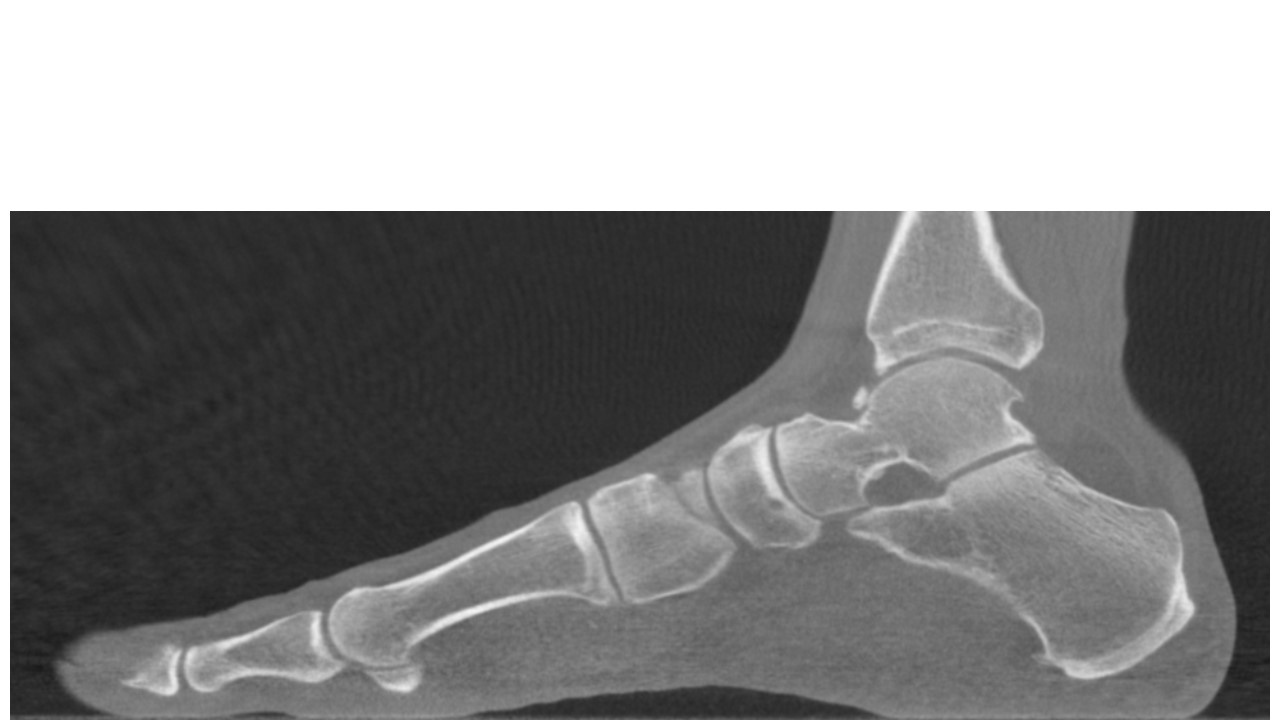

Standing CT scanning showing bone spurs arising from the anterior tibial joint margin and below on the head-neck junction of the talus.
Dynamic ultrasound evaluation can be useful to determine which positions provoke impingement, to assess blood flow in inflamed tissue using colour doppler flow examination and any surrounding tendonitis which may mimic impingement. Ultrasound can also be used to accurately target joint injections.
Non-Surgical Treatment
With an acutely inflamed ankle a period of rest and immobilization with an offloading ankle boot or brace can be very helpful. This coupled with simple painkillers and an oral anti-inflammatory such as ibuprofen will resolve most acutely painful exacerbations.
It is then important to work-out which positions are causing impingement and to alter activity or foot position to guard against triggering the pain. A simple semi-rigid insole or a shoe with a raised heel of rocker-soled shoe may be helpful in certain patients.
Physiotherapists are very important in managing impingement. If there is ankle instability then muscle strengthening and balancing techniques and sometimes taping or bracing of the ankle to prevent extremes of ankle position can be the difference between getting through a sports match and not.
A targeted injection of local anaesthetic and steroid can be useful to settle a painful exacerbation of impingement but it is important this is not done on a regular basis. Repeated steroid injections can be harmful to a young adults ankle cartilage.
Surgical Treatment
Most anterior ankle joint bone spurs can be removed using “key-hole” (arthroscopic) surgery which is usually carried out as a day case. This type of surgery is very common and offers very good results provided the rest of the ankle joint is in good condition.
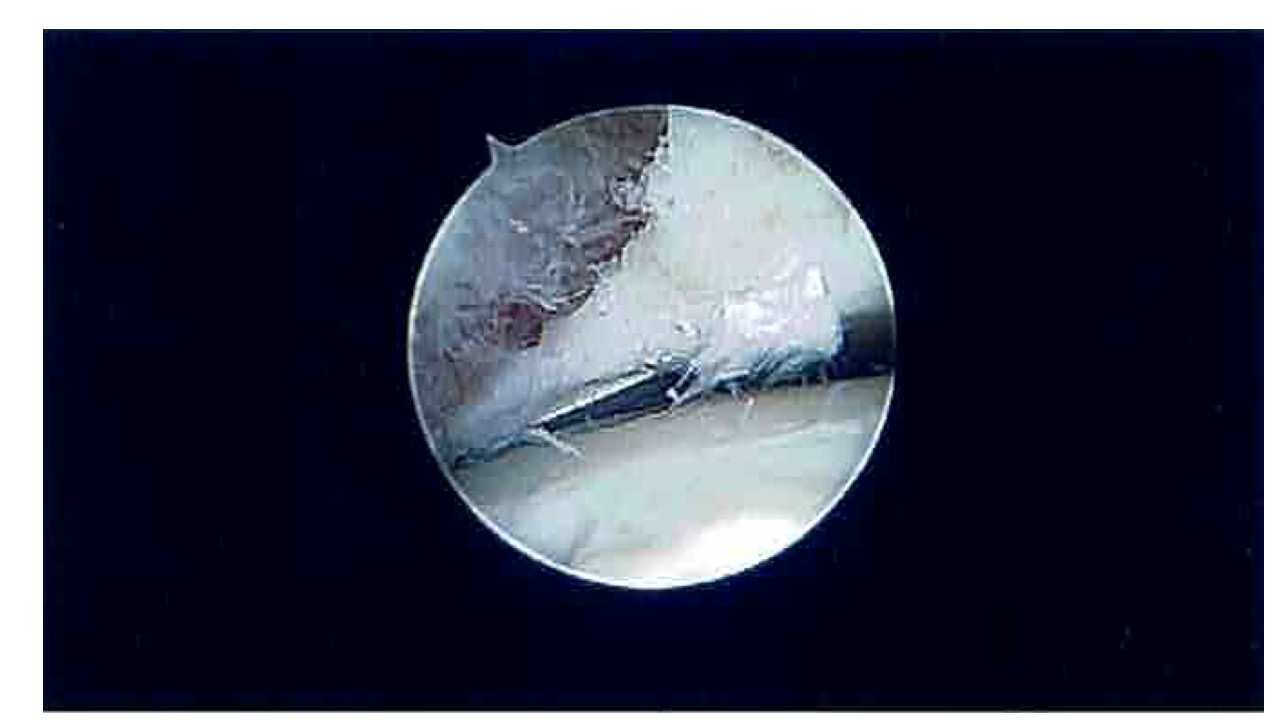

Before and after pictures of an anterior ankle bone-spur removed with an arthroscopic burr.





