- Ankle Arthritis
- Anterior Ankle Impingement and Bone Spurs
- Posterior Ankle Impingement and Os Trigonum
- Ankle Fracture
- Ankle Instability
- Ankle Syndesmosis Injury
- Osteochondral Lesions of the Talus (OLT)
- Tibialis Posterior Tendon Dysfunction
- Plantar Fasciitis
- Hindfoot Arthritis
- Lesser Toe Deformity
- Achilles Tendon Disorders
- Achilles Tendon Rupture
- Peroneal Tendon Disorders
- Calf Strain
- Ganglions
Ankle Fracture
What is it?
Fractures around the ankle can take-on various configurations but roughly there are two main groups- malleolar fractures, caused by low-energy and high energy, “Pilon Fractures” which are a unique group as they are often accompanied by severe soft tissue injury and are therefore best managed by a team of “orthoplastic” surgeons in major trauma centres. By far the more common injury is the malleolar ankle fracture.
What is it caused by?
Patients most often comment that they “turned-over” the ankle or simply twisted-it playing sport. The mechanism of injury is that of a severe ankle sprain making these injuries undistinguishable. Thorough clinical evaluation is therefore strongly advised with persistent ankle pain and swelling after an injury.
Symptoms
Patients will likely have significant swelling around the ankle with pain and tenderness on the bony prominences around the ankle. It is difficult to weight bear on ankle fractures if they are unstable and so this alone should prompt a visit to the emergency department for imaging. Bruising appears late and will often be remote from the fracture since blood tracks with gravity and so it is common to see bruising as far back as the heel.

Diagnosis
Simple plain X-rays are usually adequate to diagnose an ankle fracture. A number of ankle fractures are stable, which means they are unlikely to displace under normal load-bearing conditions. To determine this, it is commonplace for weight-bearing X-rays to be carried-out, usually a few days after the acute injury.
Sometimes a CT scan may be needed if a fracture, obviously requiring operative intervention needs further planning studies.

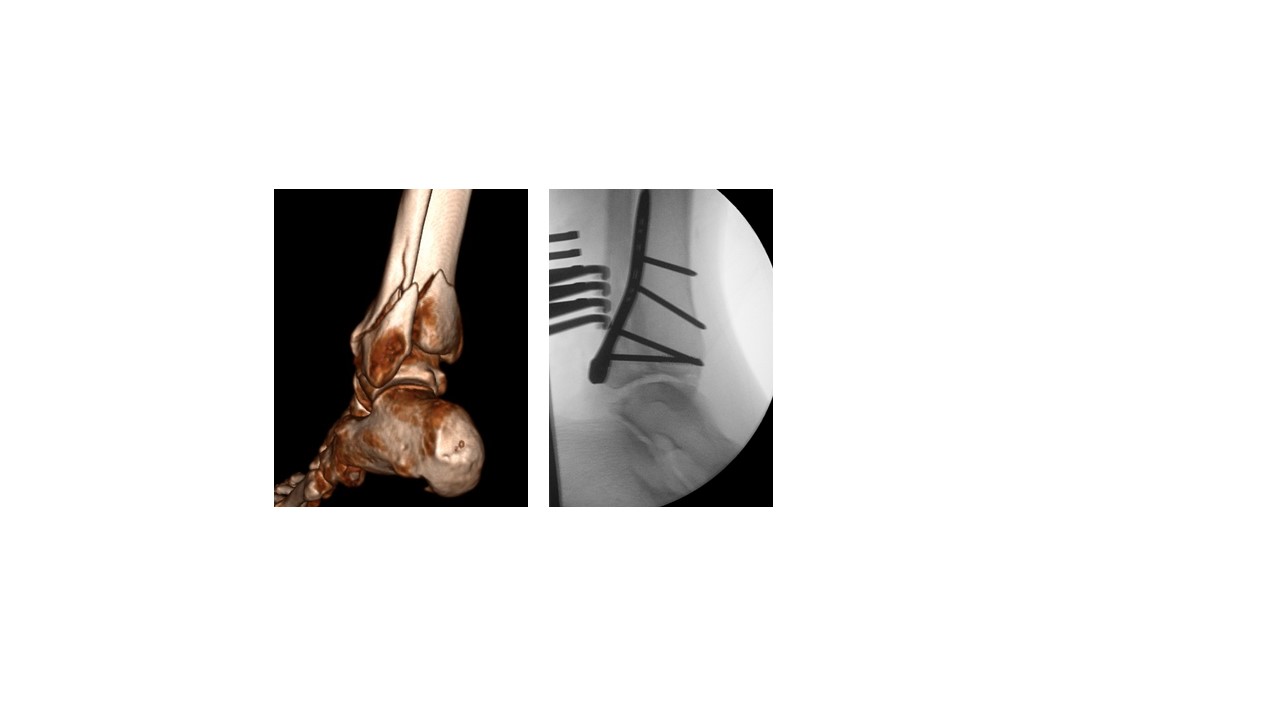
Fairly innocent-looking medial and lateral malleolar fractures on the A-P (frontal) X-ray view but the lateral projection reveals the ankle joint to be partially dislocated (subluxated). A CT scan was used to plan the surgical fixation from the back of the ankle joint.
Non-Surgical Treatment
Provided certain conditions are met it is common for ankle fractures to be treated non-operatively. You will be told at each stage in your recovery, whether or not to weight-bear and if your leg requires immobilization in plaster, or a walker-boot.
Whether or not you have surgery, your mobility will be significantly restricted. It is likely you will need some time off work to elevate your leg at home and reduce swelling while taking pain-killers. You will be asked whether you have ever had a Deep Vein Thrombosis (DVT) or Pulmonary Embolism (DVT) and depending on your risks for this you might be asked to self-administer an anti-coagulant injection or tablet for the period of time that you are non-weight-bearing and immobilized.
Flying or traveling long distances by other means is not recommended. Rest is important for your recovery and flying increases the risk of limb swelling and DVT.
As time progresses and your fracture unites, it will be important to transition you to weight-bearing and normal walking and so physiotherapy towards the end of your treatment will be implemented.
Surgical
Surgery for ankle fractures is indicated where there is obvious instability, especially if your ankle had to be manipulated or “reduced” into position before it was placed in plaster. Fractures extending into the ankle joint most commonly undergo surgery to avoid unevenness in the joint which would risk the development of early onset ankle arthritis.
The timing of surgery is important. When you sustain an ankle fracture the soft tissues will swell, making early surgery risky and wounds prone to breaking-down. Waiting too long can make the surgery technically challenging and so the ideal period is roughly between 5 and 14 days.





